Autoimmune manifestation in splenic atrophy presented with toxic shock syndrome: a case report
Abstract
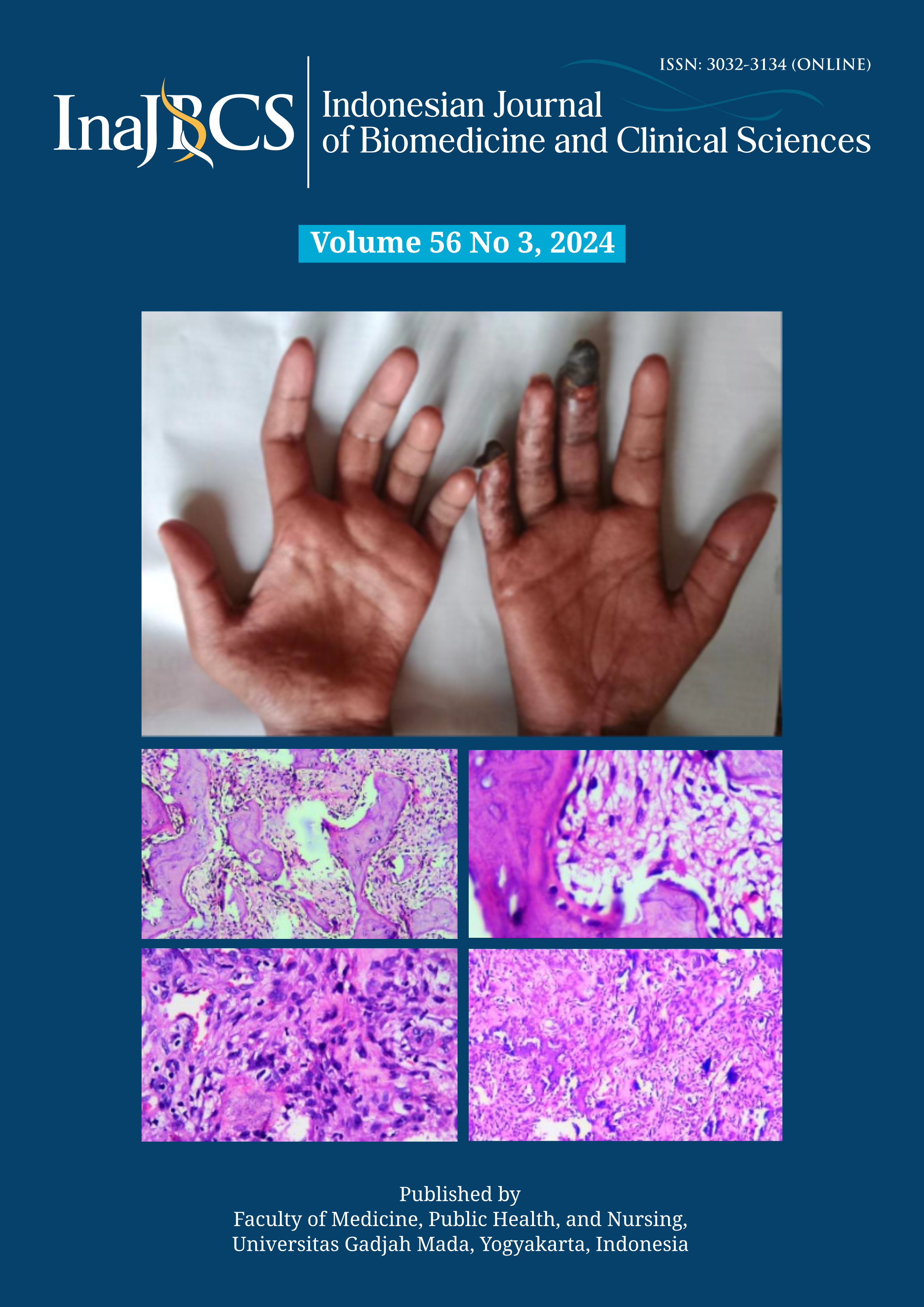
Splenic atrophy is an uncommon diagnosis, associated with autoimmune gastrointestinal disorders and other well-characterized connective tissue diseases. We would like to contribute a case report to support the association evidence of the real-world data. To our best knowledge, there is no similar case of splenic atrophy with the presentation of streptococcal toxic shock syndrome reported. Our patient was initially detected with atrophic spleen via CT scan and subsequently diagnosed with systemic sclerosis. Hyposplenism should be suspected in patients with adult-onset infections caused by encapsulated bacteria, especially if autoantibodies are present. Our patient received her pneumococcal vaccination before discharge and was followed in the clinic for further vaccination education and health check-up. Learning points: 1) Acquired splenic atrophy is a rare condition that may be suspected from persistent isolated thrombocytosis after the resolution of sepsis and Howell-Jolly bodies from peripheral blood film; 2) The pathophysiological mechanism of splenic atrophy in the context of autoimmune disorders remains unknown; 3) A high index of suspicion towards the evaluation of splenic function is required if a patient presented with community-acquired encapsulated organism bacteraemia; 4) Vaccination against encapsulated bacterial agents should be performed in patients with hyposplenism.
References
Malpighi, M. De liene. Quoted in: Sotgiu et al. Celebrazioni Malpighiane. Discorsi e scritti, Bologna, 1965; 24.
Mebius RE, Kraal G. Structure and function of the spleen. Nat Rev Immunol 2005; 5(8):606-16.
https://doi.org/10.1038/nri1669
Di Sabatino A, Carsetti R, Corazza GR. Post-splenectomy and hyposplenic states. The Lancet 2011; 378(9785):86-97.
https://doi.org/10.1016/S0140-6736(10)61493-6
Di Sabatino A, Carnevale Maffè G, Brunetti L, Guerci M, Corazza GR. Splenic hypofunction in patients with an incidental finding of small-sized spleen at abdominal ultrasound. Intern Emerg Med 2013; 8(4):361-2.
https://doi.org/10.1007/s11739-012-0869-7
Rokkam VR, Kotagiri R. Secondary thrombocytosis. In: StatPearls. StatPearls Publishing, Treasure Island (FL); 2022.
Hachulla E, Launay D. Diagnosis and classification of systemic sclerosis. Clin Rev Allergy Immunol 2011; 40(2):78-83.
https://doi.org/10.1007/s12016-010-8198-y
Santos N, Silva R, Rodrigues J, Torres-Costa J. Sjögren’s syndrome and acquired splenic atrophy with septic shock: a case report. J Med Case Rep 2014; 8:10.
https://doi.org/10.1186/1752-1947-8-10
Fishman D, Isenberg DA. Splenic involvement in rheumatic diseases. Semin Arthritis Rheum 1997; 27(3):141-55.
https://doi.org/10.1016/s0049-0172(97)80013-3
Coppo P, Saadoun D, Varet B. Autoimmune manifestations in acquired idiopathic splenic atrophy: a puzzling association. Eur J Intrn Med 2006; 17(8):580-2.
https://doi.org/10.1016/j.ejim.2006.07.008
Lookwood CM, Worlledge S, Nicholas A, Cotton C, Peters DK. Reversal of impaired splenic function in patients with nephritis or vasculitis (or both) by plasma exchange. N Engl J Med 1979; 300(10):524-30.
https://doi.org/10.1056/NEJM197903083001003
Wardrop CA, Dagg JH, Lee FD, Singh H, Dyet JF, Moffat A. Immunological abnormalities in splenic atrophy. The Lancet 1975; 2(7923):4-7.
https://doi.org/10.1016/s0140-6736(75)92949-9
Wessels MR. Capsular polysaccharide of group A Streptococcus. Microbiol Spectr 2019; 7(1):10.1128/microbiolspec.GPP3-0050-2018.
https://doi.org/10.1128/microbiolspec.GPP3-0050-2018
Boyle S, White RH, Brunson A, Wun T. Splenectomy and the incidence of venous thromboembolism and sepsis in patients with immune thrombocytopenia. Blood 2013; 121(23):4782-90.
https://doi.org/10.1182/blood-2012-12-467068
Lee DH, Barmparas G, Fierro N, Sun BJ, Ashrafian S, Li T, et al. Splenectomy is associated with a higher risk for venous thromboembolism: a prospective cohort study. Int J Surg 2015; 24(Pt A):27-32.
https://doi.org/10.1016/j.ijsu.2015.10.011
Bonanni P, Grazzini M, Niccolai G, Paolini D, Varone O, Bartoloni A, et al. Recommended vaccinations for asplenic and hyposplenic adult patients. Hum Vaccin Immunother 2017; 13(2):359-68.
https://doi.org/10.1080/21645515.2017.1264797
Rubin LG, Levin MJ, Ljungman P, Davies EG, Avery R, Tomblyn M, et al. 2013 IDSA clinical practice guideline for vaccination of the immunocompromised host. Clin Infect Dis 2014; 58(3):309-18.
https://doi.org/10.1093/cid/cit816
Kanhutu K, Jones P, Cheng AC, Grannell L, Best E, Spelman D. Spleen Australia guidelines for the prevention of sepsis in patients with asplenia and hyposplenism in Australia and New Zealand. Intern Med J 2017; 47(8):848-55.